The Irish media is full of horror stories about patients waiting for days on trolleys and growing waiting lists. These descriptions often include expressions like “underfunded” or “due to cutbacks’, giving the impression that the problems are due to lack of funding. There’s an unspoken belief that we could have French standards of health service if we increased our expenditure to French levels.
My interest in health care expenditure started, bizarrely, on a taxi journey up O’Connell Street in 2002, when the Spire was under construction. The taxi driver complained about the cost of the Spire and how many hospital beds could be provided instead. I love a good statistic so I simply had to find this out. In those pre-Smartphone days, I had to wait to get home to find the data. When I did the maths, it turned out the total cost of building the Spire (€4M) would have kept the health service going for less than 4 hours in 2002.
We spend a lot of money on healthcare. The health budget in 2015 was just under €20b which represents about 27% of all government expenditure. This amounts to about €4000 per year for every man, woman and child in the country.
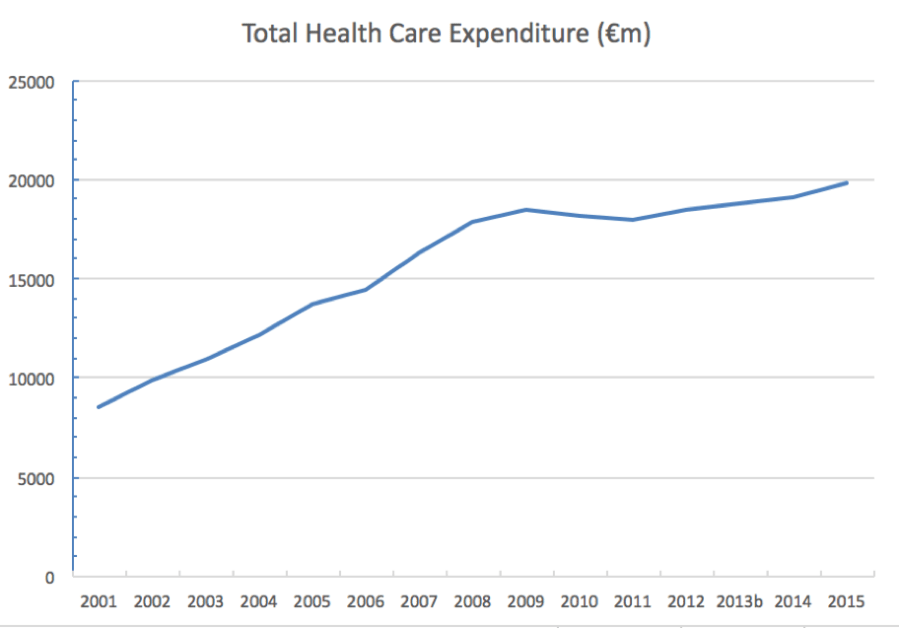
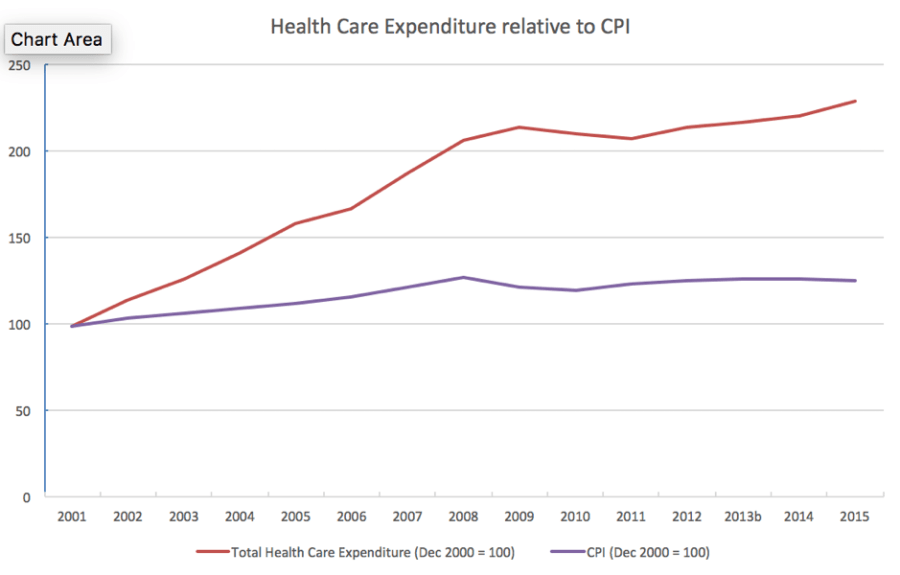
Current spending is more than double the €9b in the we spent in 2002. You can see a slight drop around 2010-11 but overall the trend has been consistently upwards, considerably outpacing increases in the Consumer Price Index.
Late in 2016, the OECD produced a comprehensive comparison of health services across Europe, with lots of different metrics. The figures for Ireland are depressing.
On a per capita basis, we’re in the top tier of European countries, spending about the same as Germany, the Netherlands, Sweden and Austria. We spend more than France, which is often lauded for the standard of its health services, and considerably more than the UK.
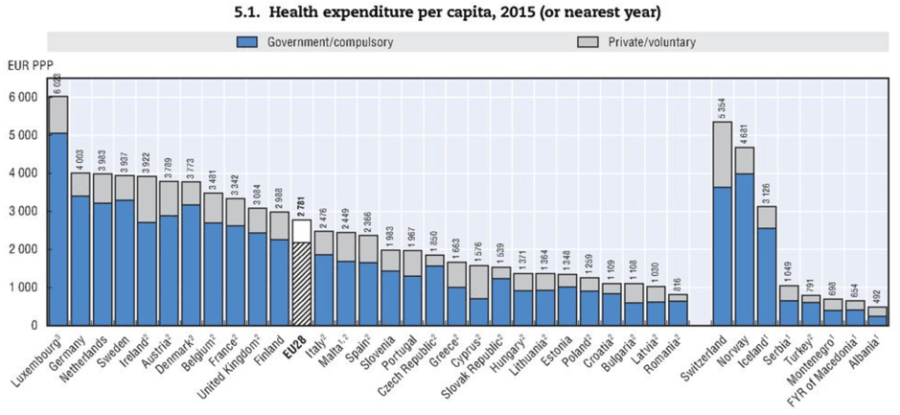
The OECD figures include both government expenditure and private expenditure. The latter covers items like private health insurance and charges for doctors and medicines which the patient has to pay themselves. In Ireland these “private/voluntary” charges amount to about €1300 per person per year in 2015, which is one of the highest costs anywhere.
But even excluding this, the amount the government pays is very substantial. The Irish government paid about €3123 per person in 2015. The UK government paid €2779 per person, but this lower amount provided free GP services and heavily subsidised (or free) prescription drugs.
And so to bed
Consultants continually complain that problems of waiting times and delays in A&E are due to a shortage of hospital beds. The international evidence suggests the hospital consultants are correct on this. In 2014, Ireland had 2.6 beds per 1000 people; only Sweden had fewer beds per capita. While the age population in Ireland is relatively youthful, it is growing in size and becoming older. In January the HSE concluded that Ireland needs an extra 2,500 to 7,500 hospital beds , through there has been no detail on how and when these will be provided.
This comparatively small number of beds is spread across 29 acute hospitals. Some of these hospitals are simply too small to offer all the specialisms you would expect. Private hospitals duplicate many public facilities.
Furthermore, what beds are available tend be in old buildings. Health planners in the Netherlands generally regard the lifespan of an acute hospital to be 40 years. In Dublin some patients in the Mater Hospital are treated in wards built in 1861. There is an increasing international practice of using mainly single bed rooms to reduce the risk of cross infection and improve the privacy and dignity of patient care but there is little progress on this in Ireland. As evidenced by the protracted controversy about the new maternity hospital on the St. Vincent’s site, the complex ownership of hospitals in Ireland, with many facilities are funded by the HSE but owned by a religious body, can complicate development.
13 hours a week for €162,319 a year
It looks like some doctors are paid a lot of money. In 2015, specialists in Ireland were paid an average salary of €162,319. This makes them the 2nd best paid in Europe after Luxembourg. Most consultants are on what are called Category B or C contracts where they also are allowed to treat and charge separately private patients outside their contractual hours. A 2017 RTÉ Prime Time programme found that some consultants worked as little as 13 hours a week in the public hospital in which they are employed, and well paid.
This system gives rise to a perverse incentive for consultants to not treat public patients so that worried patients will skip the queue by attending as a private patient.

Sunday Business Post journalist Oliver O’Connor of the has found that a hip operation costs twice as much to perform in an Irish hospital as in the UK. This may be at least partly due to the small average size of our hospitals, but the rates of pay must also be a factor.
The average salary may however mask a division between those specialists appointed before and after 2012, when significant cuts in starting salaries were applied. [Consultant contracts: costly question for the next government] 15% of consultant posts are unfilled due to recruitment difficulties, reportedly because the new salaries are lower than those available elsewhere.
The OECD does not publish figures for specialists in Australia or Canada and has very limited such data for the USA. What it does show is that in the USA in 2001, the average specialist salary was $170,300, far higher than any other country at that time. Assuming that the US has retained this lead, could the paradox of recruitment difficulties despite, by European standards, high salaries be due to emigration to the US? A monoglot French doctor has fewer opportunities to practice in another rich country than a monoglot English-speaking Irish doctor.
The drugs don’t work
We also seem to spend a lot on medicines, second only to Germany in the EU. The OECD figures don’t indicate whether this is due to high costs of drugs in Ireland or more medicines being prescribed.

And wait we do
There are many things our health service does well. It seems to be much quicker to get an appointment with a GP in Ireland than, for example, the UK.
The Euro Health Consumer Index 2017 published by Swedish think tank the Health Consumer Powerhouse, rates Ireland worst in Europe for access to specialists. The (very readable) report comments archly that “…the programme initiated to reduce healthcare waiting times in Ireland aims at a target of no more than 18 months’ (!) wait for a specialist appointment. Even if and when that target is reached, it will still be the worst waiting time situation in Europe.”
The Health Consumer Powerhouse report doesn’t provide metrics on A&E waiting times but these can be inferred from other sources.
In February 2017, 10% of NHS England A&E patients had to wait more than 4 hours before discharge or admission.
The HSE doesn’t publish figures for 4 hours, but their figures indicate that, in the same month, 19.5% of A&E patients in Ireland waited more than 9 hours and 3.9 % more than 24 hours. By a very rough estimate, about 10% of patients in Ireland waited more than 12 hours, three times longer than the equivalent number in England.
Any family history of this condition?
While other sectors have benefitted from IT investment, the doomed PPARS project in the noughties seems to have left a legacy of avoiding IT solutions in the health service.
It also appears that some of the efficiencies which were supposed to be delivered as a result of the merger of the 11 old health boards into the HSE have never materialised. (At this point, I should point out that the oft-quoted fact that we had 11 health boards for a country with fewer people than Greater Manchester is simply not true, as discussed in another blog post.)
The Health Consumer Powerhouse notes that in Macedonia “since July 2013, any GP can call up the booking situation of any specialist or heavy diagnostic equipment in the country in Real Time with the patient sitting in the room, and book anywhere in the country with a few mouse clicks.” In Ireland with a per capita GDP 12 times larger and a thriving tech sector, appointments are requested by letter, which aren’t even always opened.
There are many reasons for the much poorer service in Ireland. Lack of money isn’t one of them.

One thought on “Myth no. 1 “We need to spend more money on healthcare””